|
|
COSMETIC SURGERY OF THE EYELIDS or
COSMETIC BLEPHAROPLASTY
DEFINITION, AIMS AND PRINCIPLES
‘Blepharoplasties’ means aesthetic surgical procedures of the
eyelids aiming to correct unsightly aspects, whether due to
heredity or age. They can be performed on the upper or lower
eyelids alone, or all four at the same time.
This technique may be carried out alone or in association with
other cosmetic facial surgery (brow-lift, forehead-lift, faceand
neck-lift) or with techniques such as laser resurfacing,
dermabrasion or chemical peels.
The goal of a blepharoplasty is to correct signs of aging and
remove the tired look due to the heavy eyelids by a more
rested, relaxed appearance.
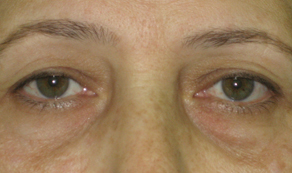
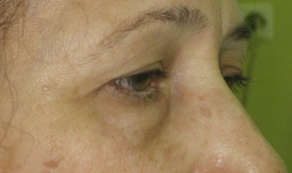
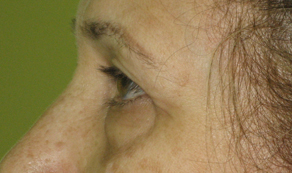
The unsightly aspects most commonly found are the
following:
Drooping heavy upper eyelids, with a more or less marked
skin-fold.
Lower eyelids which have drooped and shrunk, leading to
horizontal wrinkles due to distended skin.
Bulging fat, responsible for ‘bags under the eyes’ at the lower
eyelid level, or sagging upper eyelids
The procedure aims to correct these problems durably by
surgical removal of excess skin, fat and muscle, without of
course affecting the normal functions of the eyelids.
This procedure, for both men and women, is often carried out
around the age of forty.
It can however be done much earlier where the problem is
congenital rather than age-related, for example in the case of
bags under the eyes.
BEFORE THE OPERATION
Prior to the operation a thorough examination of the eyes and
eyelids will have been carried out in order to detect any
anomalies which could complicate the procedure or indeed
show that it is not recommended in this specific case.
A specialised ophthalmologic examination will often be
prescribed to rule out any ocular pathology.
HOSPITAL STAY AND TYPE OF ANESTHESIA
Type of anesthesia
Local anesthesia with sedation given by intravenous drip. (‘twilight’ anesthesia)
Hospital stay
The procedure may be carried out on an out-patient basis, in
an ambulatory facility, the patient leaves on the same day
after a few hours under observation.
THE PROCEDURE
Incisions
 Upper eyelids: They are
concealed in the fold
situated at the mid-point
of the eyelid, between the
mobile and fixed parts. Upper eyelids: They are
concealed in the fold
situated at the mid-point
of the eyelid, between the
mobile and fixed parts.
Lower eyelids: They are
1 to 2mm below the
eyelashes, and can go
slightly beyond them.
Note : For the lower eyelids, in the case of isolated “bags” (without excess skin to be removed), a blepharoplasty can be carried out by the transconjunctival approach, that is by using incisions placed inside the eyelids, thus leaving no visible
scar.
Resection : Once the incision made, unsightly excess fat is
removed, as are redundant muscle and sagging skin.
Sutures : Stitches are made using very fine nonabsorbable
thread (they are removed a few days after the procedure).
The operation can take between 30 minutes and 2 hours
depending on the specific requirements and complexity of the
case.
AFTER THE OPERATION
There is no actual pain, but possibly some discomfort with a
sensation of tension in the eyelids, slight irritation of the eyes
and perhaps some blurring of vision.
During the first few days rest is advised, with no physical
strain, no lifting heavy weights for example.
During the recovery period there will be edema (swelling),
and bruising, to a variable degree for each individual patient.
For the first few days it may be impossible to close the eyes
completely, a slight detachment of the external angle of the
eye may also be observed, but in both cases these signs are
rapidly reversible.
The sutures will be removed between the 3rd and 6th day after
surgery.
Visible signs of the operation will diminish little by little, a
return to normal social and professional activities will be
possible after 6 to 20 days.
The scars may remain as pinkish lines for the first few weeks,
but can be hidden by makeup from the 7th day onward.
Slight hardening of the detached zones may persist for a few
months, but is not perceptible to others.
THE RESULT
The final aspect will not be visible before 3 to 6 months. This
is the time lapse necessary for the tissues to regain their
softness and for the scars to heal and practically disappear.
The results of this procedure are usually among the most
durable found in aesthetic surgery. Once the fatty pads
removed they do not in general return, so this is a permanent
effect.
DISAPPOINTING RESULT
These can result from a misunderstanding concerning what
can reasonably be achieved. For example lowering of the
forehead and eyebrows can only be corrected by a foreheadand
brow-lift.
They can also be due to unexpected tissue reaction or unusual
scarring phenomena.
Very fine lines may persist, the eyes may appear slightly too‘hollow’ (the bony outline of the eye-socket being visible).
Other imperfect results could be a slight downward retraction
of the lower eyelids, slight asymmetry, or ‘whitish’ scars.
These imperfections can be remedied by corrective surgery if
necessary, usually under local anesthesia from the 6th month
following surgery.
POSSIBLE COMPLICATIONS
Fortunately, real complications are rare following a
blepharoplasty which has been carried out correctly. In fact
practically all the operations go well and patients are
completely satisfied with the result.
In spite of the fact that complications are so rare you must be
aware of the following possible problems :
- Hematomas: not usually serious, they can be
drained if necessary.
- Infections: extremely rare for this procedure, microabscesses
can develop on stitches but are easily
treated. Conjunctivitis will be prevented by routine
prescription of eye-drops for the first few days after
the procedure.
- Abnormal scarring: this is very rare for the eyelids
where the skin usually heals leaving almost no trace
of surgery, the scars can however sometimes be
more pronounced than hoped.
- Epidermal cysts: they can appear along the scars,
but often clear spontaneously, if not they can easily
be removed and do not affect the final result.
- Lacrymal problems: excessive tear production is a
rarer problem than ‘dry eye syndrome’ which can
decompensate a pre-existing lack of tear production.
- Ptosis: (Drooping of the upper eyelid) : this is very
rare except in the over 70’s where a pre-existing
problem can be made worse by the operation.
- Lagophthalmos: (inability to close the upper eyelid
completely) : this can occur for the first few days
after surgery but should not persist after a few
weeks.
- Ectropion: (lower eyelid retraction) : the severe
form is extremely rare following this procedure
when it is carried out correctly. The minor form can
occur when lax tissue is affected by excessive scar
retraction; it usually recedes after several weeks of
regular massage which improves the tonus of the
eyelids.
All things considered, the risks must not be overestimated,
but you must be conscious that an operation, even a minor
one, always has some degree of unforeseeable unknown
factors.
|